Cardiology Clinic Improves First-Visit Diagnostic Accuracy by 22%

An internal blinded chart review at Vanguard Internal Medicine showed higher-than-benchmark diagnostic miss rates in complex cases. Leadership chose to address the issue before it escalated into external review risk.
Business Challenges
The internal blinded chart review at Vanguard Internal Medicine in late 2024 was part of a long-running annual quality process at the 14-physician multi-subspecialty internal medicine group. Over six years, the results showed a gradual decline in diagnostic performance. The miss rate for complex presentations increased from 4.1% in Year 1 to 7.8% in Year 6. The top-3 differential accuracy metric declined from 91% to 88%. While still managed internally, the trend had not been formally escalated beyond clinical leadership.
CMO Dr. Owen Sebastiani reviewed the findings with the external consultant and noted a broader industry pattern. As subspecialists increasingly managed cross-specialty presentations, diagnostic uncertainty was rising. Cases often involved overlapping symptoms across cardiology, endocrinology, neurology, and rheumatology, making consistent diagnosis more difficult. In many cases, the reasoning behind clinical decisions was not fully captured in documentation, limiting downstream clarity.
The concern for leadership was not the current performance level, but the direction of the trend. Continued decline could increase exposure during audits and raise clinical and contractual risk. The decision was made to implement diagnostic decision support before external visibility forced corrective action.
- Blinded chart review showed diagnostic miss rate increasing from 4.1% to 7.8% over six years; top-3 differential accuracy declined from 91% to 88%.
- Subspecialists increasingly managed cross-domain cases, contributing to higher diagnostic complexity and uncertainty.
- Referrals ran 18% above peer benchmark, increasing cycle time for diagnosis and resolution.
- Clinical reasoning was inconsistently documented, limiting continuity for downstream providers.
- Junior physicians lacked structured access to senior diagnostic reasoning patterns.
Solution
Procurement was led directly by Dr. Sebastiani with a clear requirement: senior physicians had to trust and adopt the system for it to work. Without clinical credibility at the senior level, adoption across the practice would not succeed.
eCareAssist’s clinical decision support platform was selected following hands-on validation with senior clinicians. In one evaluation session, Dr. Margaret Lin, a senior endocrinologist with over 30 years of experience, reviewed 14 historical complex cases alongside the platform’s diagnostic suggestions. The system’s top-three differential suggestions aligned with her clinical reasoning in 13 out of 14 cases. In one case, it surfaced a differential she acknowledged she had not initially considered. This validation was a key turning point in selection.
A second capability influencing adoption was structured documentation of diagnostic reasoning. The platform captured differentials considered, supporting evidence, and rationale for prioritization directly within the clinical workflow. This created a consistent record for care continuity and strengthened defensibility in case of external review.
Value Delivered
Improvements were reflected in the following year’s blinded chart review, showing a clear reversal in trend. Diagnostic performance returned to and exceeded earlier baseline levels, with improved consistency across complex cases.
- Top-3 differential accuracy improved from 88% to 96% in blinded review.
- Specialty referrals decreased by 24% due to improved in-visit diagnostic resolution.
- Structured reasoning capture reached 100% of complex encounters.
- Junior physicians gained access to senior-level diagnostic reasoning patterns during care delivery.
- Clinician relevance score reached 4.8/5 for recommendation quality.
Solution Provided
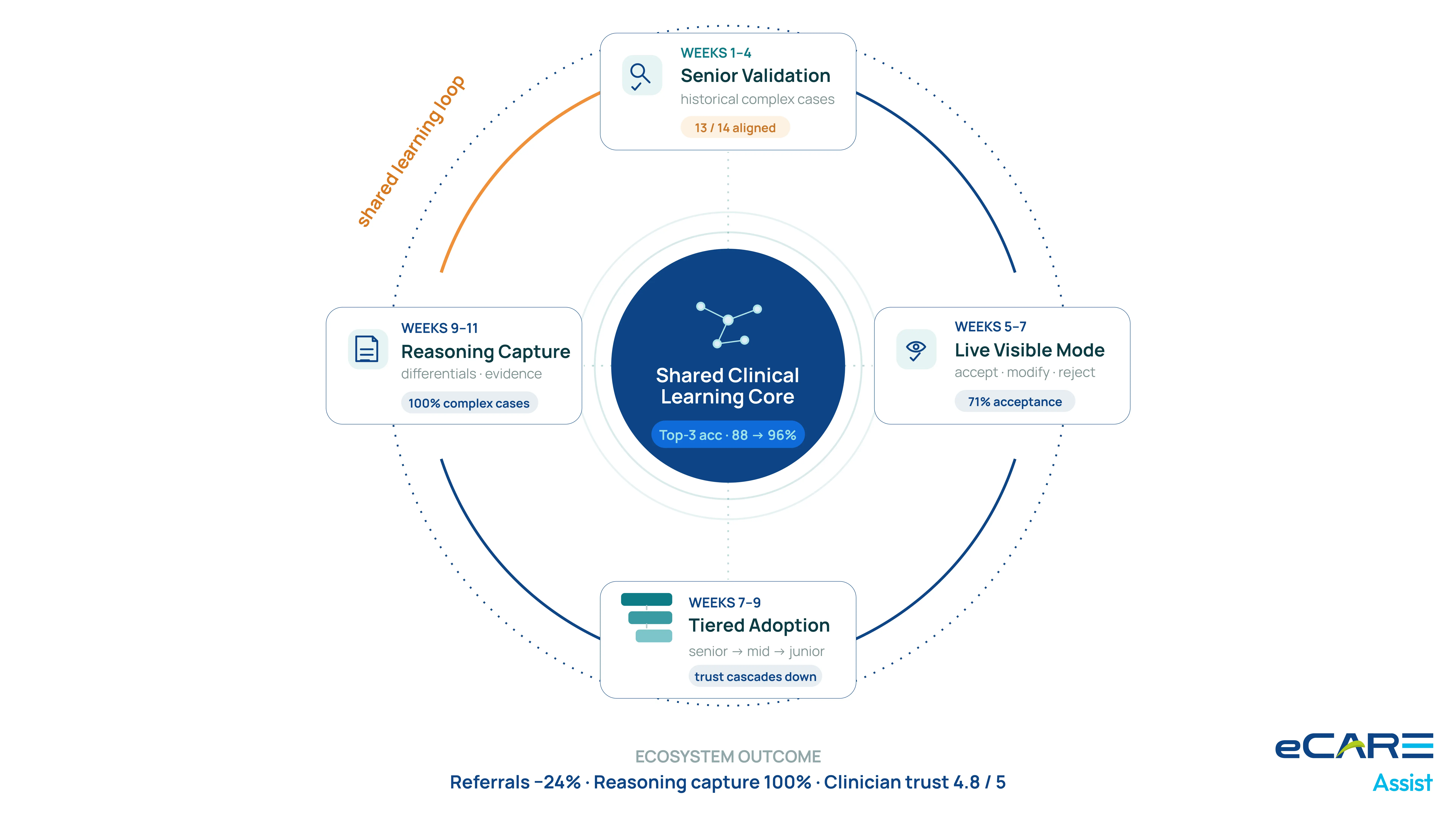
The deployment was completed over 11 weeks, structured primarily around clinical validation and trust-building among senior physicians before full-scale rollout.
Weeks 1–4: Senior Physician Validation
Senior physicians reviewed historical complex cases using the platform in guided sessions. Each case was compared against the system’s diagnostic output to assess clinical alignment. By the end of this phase, senior clinicians confirmed the system was clinically credible and aligned with accepted reasoning patterns.
Weeks 5–7: Visible-Mode Deployment for Senior Physicians
Senior physicians used the platform in live clinical settings. They could accept, modify, or reject diagnostic suggestions. Acceptance rates averaged 71%, reflecting meaningful alignment even among highly experienced clinicians.
Weeks 7–9: Mid-Career and Junior Physician Adoption
Mid-career and junior physicians were onboarded in phases. Adoption accelerated due to prior validation from senior clinicians, which established trust in the system’s recommendations.
Weeks 9–11: Structured Documentation Workflow
The final phase enabled structured capture of diagnostic reasoning. The documentation was reviewed by leadership for quality improvement and used as a teaching resource for ongoing clinical education.
Business Value
Dr. Sebastiani presented outcomes to the partner group in early 2026. The focus shifted from immediate performance gains to long-term stabilization of diagnostic quality and reduction of external risk exposure.
What the engagement preserved
The diagnostic trajectory has stabilized and improved. The organization strengthened its clinical quality position, reduced variability in complex diagnoses, and improved consistency across providers. The improvement also reinforced payer and clinical-legal positioning by reducing unresolved diagnostic variability over time.
The financial picture
Reduced external referrals resulted in approximately $880K in retained annual revenue. Improved diagnostic efficiency and reduced repeat workups contributed an additional $420K. Total annual financial impact is approximately $1.3M against a $310K implementation cost.
What changed about diagnostic reasoning as a discipline
Diagnostic reasoning is now systematically captured and shared across the organization. Junior physicians have structured access to senior-level reasoning patterns during care delivery. Monthly case reviews have evolved into structured learning sessions supported by real clinical data from the platform.
The CMO’s framing
“We identified a trend early that could have become a larger issue over time. The platform did not replace clinical judgment. It made senior reasoning visible and usable across the organization. The improvement in diagnostic accuracy is important, but the long-term value is the shared clinical learning system.”
— Dr. Owen Sebastiani, CMO, Vanguard Internal Medicine

