ACO Uses AI Risk Stratification to Capture $11M in Shared Savings

Year-one shared savings at Crestwood ACO ended at $3.1M, below the $7M actuarial forecast. Leadership linked the shortfall to issues in risk stratification.
Business Challenges
The shared-savings reconciliation was completed in late summer 2025. Crestwood Health Partners, a Medicare Shared Savings Program ACO managing 64,000 attributed beneficiaries across the Northeast, had projected $7M in year-one shared savings. The final result was $3.1M, which led the board to question the performance gap.
CMO Dr. Pradeep Mehra identified the core issue in the risk stratification approach. The ACO relied on claims-based models with a 3–4 month delay. As a result, patients were often marked high-risk only after key clinical events had already taken place. Care teams were working with outdated information instead of current patient status. While care interventions were still effective, they often came too late to prevent escalation.
Other metrics supported this view. HCC capture was at 84% of expected levels, showing missed documentation and lost risk-adjustment revenue. Annual wellness visits and chronic care management billing were under by about $1.4M. Care managers did not have a clear way to prioritize patients and were managing large lists without strong risk signals. Care was being delivered, but not always to the patients who needed it most.
- Year-one shared savings came in at $3.1M vs $7M projected — a $3.9M gap.
- Risk stratification ran on claims-based data with a 3-to-4-month lag; high-risk identification was happening after the high-risk event had already occurred.
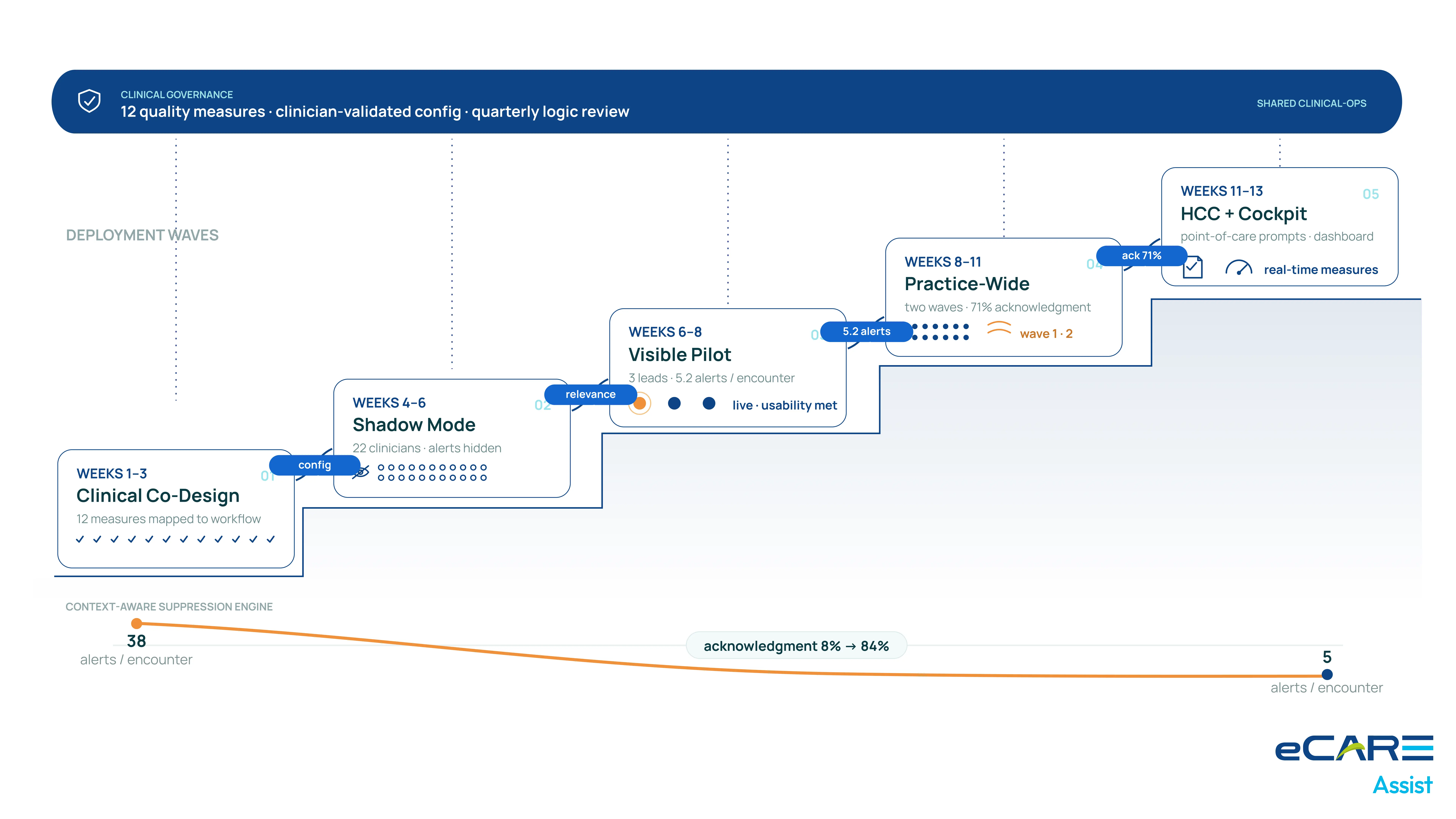
- HCC capture ran at 84% of expected; documentation precision gaps left risk-adjustment payments on the table.
- Annual wellness visit and chronic-care management billing was under-captured by ~$1.4M annually.
- Care managers were working without an effective prioritization signal — measure-chasing across dozens of beneficiaries without differential focus.
Solution
Planning for year two focused on improving speed of risk identification. To meet shared-savings goals, the ACO needed real-time insights instead of delayed claims data. Vendors without real-time capability were not considered.
eCareAssist’s clinical decision support platform was selected for its continuous risk model. Instead of relying on claims, it used live ambulatory visits, lab results, and care management data. Risk scores updated within hours of new activity, replacing the 3–4 month delay. This allowed care teams to act earlier, before patients moved into high-risk stages.
A key factor was its point-of-care HCC capture workflow. The system flagged documentation gaps during visits and provided simple prompts inside the provider workflow. These suggestions helped clinicians improve documentation during the visit instead of after it.
Value Delivered
Year-two shared savings reached $8.4M, above the $7M original target and well above the $5.5M year-two forecast. Leadership noted that earlier limits were due to data delays, not care quality.
- Year-2 shared savings of $8.4M vs $3.1M in Year 1 — a $5.3M year-over-year lift.
- Real-time risk stratification replaced the 3-month claims-based lag; care managers worked on current data.
- HCC capture rate lifted from 84% to 96% through point-of-care documentation specificity prompts.
- $1.4M of CCM and AWV billing recovered through platform-surfaced billable-encounter opportunities.
- Top-quartile performance on all quality measures attributed to the ACO for the reporting year.
Solution Provided
The rollout was completed in 18 weeks and aligned with the Year-2 performance period. The platform was fully active for about nine months of the year.
Weeks 1–4: Data Source Integration
Integration connected five PCP EMR systems, the ACO care management platform, state HIE ED data, and CMS claims feeds. Once connected, the system began generating risk scores. These were checked against historical claims data to confirm alignment.
Weeks 5–9: Care Manager Workflow Migration
Care teams moved from monthly static reports to continuous risk updates. Daily rising-risk alerts replaced old batch reports. Teams needed training and adjustment to shift from delayed data to real-time signals.
Weeks 10–13: Point-of-Care HCC Workflow at PCP Network
HCC prompts were deployed across 28 PCP practices. The rollout was designed to fit into existing workflows. Early concerns about alert fatigue were addressed by limiting prompts to cases where documentation gaps mattered most.
Weeks 14–16: CCM and AWV Billing Workflow
CCM and annual wellness visit workflows were activated. The system identified eligible patients and scheduling opportunities. Practice teams used this to improve capture of missed billing opportunities.
Weeks 16–18: Quality Measure Performance Cockpit
The performance dashboard launched in week 16. Leadership used it to track results across 28 PCP practices. Underperforming areas were quickly identified, allowing targeted follow-up within days.
Business Value
Dr. Mehra presented the Year-2 results to the board in late 2025. The discussion shifted toward where similar real-time insights could be applied across other areas of operations.
What the engagement changed about Crestwood’s value-based-care thesis
Year-one results raised concerns about whether the shared-savings model worked at scale. Year-two results showed the issue was not care quality, but lack of real-time data. After this, the board approved expansion into two-sided risk arrangements for fiscal 2026, a decision not supported after year one.
The financial picture
The $5.3M year-over-year improvement is the main gain. HCC improvements add about $2.8M in risk-adjustment value. CCM and AWV improvements add around $1.4M. Total annual impact is about $9.5M against a $720K implementation cost, with continued growth expected as risk-based contracts expand.
What changed about care management as a discipline
Care management at Crestwood shifted from reacting after events to acting earlier based on risk signals. Teams now focus on patients before conditions worsen, not after.
The CMO’s framing
“The care team was strong, but working with delayed and incomplete data. Year-one results reflected a data problem, not a care problem. Once the data improved, the care model performed as expected.”
— Dr. Pradeep Mehra, CMO, Crestwood Health Partners

